doi: 10.62486/agmu202465
ORIGINAL
Sex differences in ST-segment elevation acute myocardial infarction
Diferencias, según sexo, del infarto agudo de miocardio con elevación del segmento ST
Anabel Sánchez Orraca1 ![]() ,
Miladys Orraca Castillo2
,
Miladys Orraca Castillo2 ![]() , Damaris Hernández Véliz1
, Damaris Hernández Véliz1
![]()
1Instituto de Cardiología y Cirugía Cardiovascular. La Habana. Cuba.
2Sociedad Científica Cubana para el Desarrollo de la Familia (SOCUDEF). La Habana. Cuba.
Cite as: Sánchez Orraca A, Orraca Castillo M, Hernández Véliz D. Sex differences in ST-segment elevation acute myocardial infarction. Multidisciplinar (Montevideo).2024; 2:65. https://doi.org/10.62486/agmu202465
Submitted: 21-11-2023 Revised: 18-04-2024 Accepted: 11-09-2024 Published: 12-09-2024
Editor: Telmo
Raúl Aveiro-Róbalo ![]()
ABSTRACT
Introduction: Acute ST-segment elevation myocardial infarction constitutes a health problem in the world and in Cuba, with differences according to sex in clinical and laboratory findings, complications and therapeutic response.
Objective: to identify sex differences in ST-segment elevation myocardial infarction.
Method: quantitative, cross-sectional, retrospective study of 155 patients, 97 men and 58 women, from the Coronary Intensive Care Unit of the Institute of Cardiology and Cardiovascular Surgery, from January 2020-December 2021. The following variables were explored: general, admission, hospitalization and complications.
Results: the following were statistically significant: men developed infarction earlier than women (65±13 vs 71±11,9); of the known coronary risk factors, arterial hypertension predominated (61,3 %); smoking prevailed in men (53 %) and 54 % of the patients with an anterior-extensive topographic location died (80 % in men and 100 % in women). In addition, there was a predominance of Killip-Kimball IV classification (15,5 %), right coronary artery as the responsible vessel (29,9 %), heart failure as a complication (26,8 %) and death (15,5 %) in men. However, in women, the anterior descending coronary artery prevailed as the vessel responsible for the lesion (34,4 %).
Conclusions: there are differences between men and women in age, risk factors and clinical manifestations of ST-segment elevation myocardial infarction. Women were more likely to present extensive anterior myocardial infarction, a topography that had a greater incidence of mortality as a complication.
Keywords: Acute Myocardial Infarction; Ischemic Heart Disease; Diagnosis; Treatment; Sex.
RESUMEN
Introducción: el infarto agudo de miocardio con elevación del segmento ST constituye un problema de salud en el mundo y en Cuba, con diferencias según el sexo en hallazgos clínicos, de laboratorio, complicaciones y respuesta terapéutica.
Objetivo: identificar diferencias, según sexo, del infarto agudo de miocardio con elevación del segmento ST.
Método: investigación cuantitativa, transversal, retrospectivo en 155 pacientes, 97 hombres y 58 mujeres, de la Unidad de Cuidados Coronarios Intensivos del Instituto de Cardiología y Cirugía Cardiovascular, de enero 2020-diciembre 2021. Se exploraron variables: generales, al ingreso, de hospitalización y complicaciones.
Resultados: se destacan, con significación estadística, que los hombres desarrollaron el infarto más temprano que las mujeres (65±13 vs 71±11,9); de los factores de riesgo coronario conocidos predominó la hipertensión arterial (61,3 %); que el tabaquismo prevaleció en los hombres (53 %) y el 54 % de los pacientes con localización topográfica anterior-extenso fallecieron (en hombres el 80 %, y en mujeres el 100 %). Además, existió predominio de clasificación Killip-Kimball IV (15,5 %), la arteria coronaria derecha como vaso responsable (29,9 %), la insuficiencia cardíaca como complicación (26,8 %) y la muerte (15,5 %) en hombres. Sin embargo, en mujeres prevaleció como vaso responsable de la lesión, la descendente anterior (34,4 %).
Conclusiones: existen diferencias entre hombres y mujeres en edad, factores de riesgo y clínica del infarto agudo de miocardio con elevación del segmento ST. Las mujeres fueron más propensas a presentar infarto anterior extenso, topografía que tuvo mayor incidencia en la mortalidad como complicación.
Palabras clave: Infarto Agudo de Miocardio; Cardiopatía Isquémica; Diagnóstico; Tratamiento; Sexo.
INTRODUCTION
Cardiovascular diseases are the leading cause of death in the world, among which ischemic heart disease is the most common type of heart disease.(1) Among them, coronary heart disease stands out. It manifests itself in different forms: angina pectoris, acute myocardial infarction (AMI) with or without ST-segment elevation, heart failure, arrhythmias, and cardiac arrest.(2)
Acute myocardial infarction is one of the most critical manifestations of coronary heart disease, a determinant of morbidity and mortality and of disability for men and women in the fifth decade of life, often permanently due to heart failure and/or angina pectoris.(2) It is the leading cause of death in Cuba and the most lethal of all cardiovascular diseases (75 % of deaths due to ischemic heart disease in the country).(3)
Because the transmural depth of necrosis cannot be accurately determined by clinical assessment, infarctions are usually classified as ST-elevation acute myocardial infarction and non-ST-elevation acute myocardial infarction.(1) ST-segment elevation myocardial infarction (transmural myocardial infarction) is myocardial necrosis associated with ECG changes such as ST-segment elevation that does not rapidly reverse when nitroglycerin is administered. Troponin I, troponin T, and CK are elevated.(4,5)
Coronary heart disease is more common in middle-aged men. Women live an average of 10 to 15 years longer than men without suffering heart disease, but as they age, they catch up with men. On the other hand, young women have a higher risk of death from a heart attack than men of the same age; the reasons for this are not clear. However, women presenting to emergency departments for chest pain are studied and treated less aggressively than men. (6)
Mortality rates due to AMI in men were consistently higher than in women in each year studied, with a male/female ratio of 1,5/1, respectively. The higher male mortality may be due, in part, to some risk factors such as smoking and excessive consumption of alcoholic beverages, which are more frequent in men.(6)
Women seem to be protected until menopause from the development of AMI, with a very low incidence in young women, and when it appears, it is usually associated with the presence of cardiovascular risk factors such as smoking and diabetes mellitus. There is little information regarding the etiology, clinical findings, and prognosis of AMI in these patients. Still, it should not be forgotten that most of the evidence on which current medical action is based has been obtained from studies with greater male participation.(5)
These data should alert professionals to the approach to AMI according to the sex of the patient. The objetive of this study is: To identify the differences, according to sex, in ST-segment elevation AMI in patients attended in the Coronary Intensive Care Unit of the Institute of Cardiology and Cardiovascular Surgery.
METHOD
An observational, retrospective, cross-sectional study was carried out to evaluate socio-demographic characteristics, personal history, clinical characteristics, and complications in patients with ST-segment elevation AMI of both sexes.
The study was conducted at the Coronary Intensive Care Unit of the Institute of Cardiology and Cardiovascular Surgery, Havana, from January 1, 2020, to December 31, 2021.
A non-probabilistic sample of 423 adult patients with ST-segment elevation AMI admitted to the Institute of Cardiology and Cardiovascular Surgery of Havana was analyzed. This sample comprised 155 severe and critical patients who attended the Coronary Intensive Care Unit, 19 years of age or older, with a diagnosis of ST-segment elevation AMI, of both sexes.
All critical and severe cases underwent all the clinical, radiological, ECG, and humoral procedures described in the protocol for caring for patients with ST-segment elevation AMI.
All the selected variables were evaluated according to sex. The mean and standard error were used as summary measures for quantitative variables, and absolute and relative frequencies were used for categorical variables.
To determine the association between qualitative variables (comparison of proportions), the Pearson Chi-square test was applied to evaluate the relationships between the different dichotomous and polytomous variables of interest in both sexes, and the t-test was used to compare quantitative means. Before this, the Kolmogorov-Smirnov normality test was performed, which tested the normal distribution of the variable to be studied. The significance level, alpha=0,05, was defined.
Box and whisker figures illustrated the results of the statistical analyses, which were performed using Statistical software V.12.
RESULTS
Of the 155 patients seen in 2019 and 2020, 97 cases were male and 58 female, for 62 % and 37 %, respectively (figure 1).
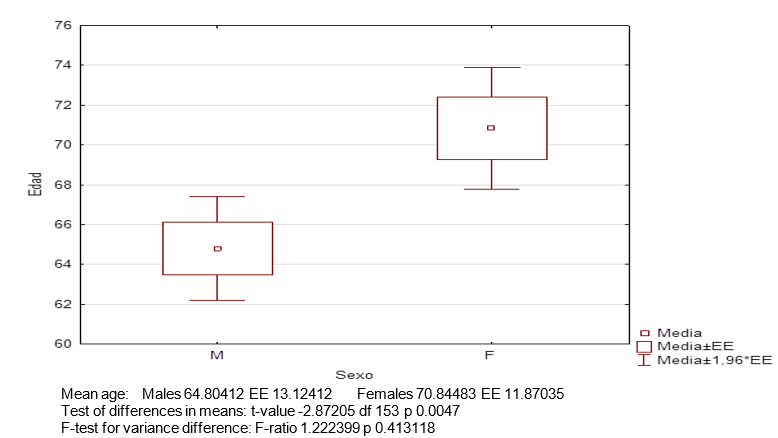
Figure 1. Mean age and standard error, according to sex, in patients with ST-segment elevation AMI. SE: standard error
Women suffered ST-segment elevation AMI at a higher age, 71 years on average, with a standard error of 11,9 years and men at 65 years with a standard error of 13 years, which implied significant differences in the mean and standard error. Thus, in this study, men presented ST-segment elevation AMI at a younger age than women.
In the analysis of the known coronary risk factors (table 1), it was found that AHT obtained a statistically significant result, so that this coronary risk factor predominated in both groups of patients.
In the case of diabetes mellitus, differences by sex were observed. Although no significant differences were found, this variable was more frequent in percentage terms in women with ST-segment elevation AMI than in men, 31 % and 17,53 %, respectively.
In this study, smoking predominated in the male sex. This factor was present in 52 of the 97 men affected with cardiovascular disease, for 53 %; however, it was present in only 32,8 % of the women. Male smokers had a significantly higher risk of ST-segment elevation AMI than female smokers, with a p-value of 0,012.
During the clinical characterization performed at admission, the most significant number were included in the first three Killip Kimball classifications, which implies that most of the patients who attended did not present cardiogenic shock. In this study, male cases performed slightly worse than female cases (15,5 % vs. 13,79 %, respectively) in the category IV classification.
In the present study, involvement was predominant in the inferior aspect of the heart (46,4 %), followed by the anterior (28,9 %) and extensive anterior.
(20,6 %) In the male sex. The highest percentages of involvement in women were also in the inferior face as topographic location (60,34 %); however, unlike men, they were followed by the extensive anterior (29,31 %) and anterior (27,59 %).
The male sex predominated in the most affected arteries; however, when it came to left central coronary artery involvement, the female sex predominated.
In the analysis of each group by sex, the artery responsible for ST-segment elevation AMI in men was the right coronary artery, followed by the anterior descending artery; however, in women, the predominant artery was the anterior descending artery, followed by the right coronary artery and the circumflex artery, with the same number of women affected. It is precisely the circumflex artery that affects men in the third order. The left main coronary artery was the most affected in women, but at the same time, it was the least affected in both sexes.
|
Table1. Characteristics of the sample studied according to sex (n=155) |
||||||
|
|
Woman n=58 |
Male n=97 |
p |
t ratio n=155 |
||
|
Age (years) + SD |
70,84 |
11,9 |
64,8 |
13 |
0,0047 |
|
|
Coronary risk factors at admission |
||||||
|
|
No. |
% |
No. |
% |
p |
T for proportion |
|
Diabetes mellitus |
18 |
31,03 |
17 |
17,53 |
0,05159 |
p<0,00001 |
|
Arterial hypertension |
36 |
62,07 |
59 |
62,11 |
0,87769 |
p=0,0061 |
|
Smoking |
3 |
5,17 |
4 |
4,12 |
0,76281 |
p=0,2981 |
|
Dyslipidemia |
3 |
5,17 |
4 |
4,12 |
0,76281 |
p<0,00001 |
|
Obesity |
2 |
3,45 |
0 |
0 |
0,06565 |
p<0,00001 |
|
Alcoholism |
0 |
0 |
3 |
3,09 |
0,17622 |
p<0,00001 |
|
Clinical classification at admission |
||||||
|
Killip Kimball I |
45 |
77,59 |
71 |
73,20 |
|
|
|
Killip Kimball II |
1 |
1,72 |
7 |
7,22 |
|
|
|
Killip Kimball III |
4 |
6,90 |
4 |
4,12 |
|
|
|
Killip Kimball IV |
8 |
13,79 |
15 |
15,46 |
|
|
|
Location of the infarction on admission, electrocardiogram |
||||||
|
Previous |
16 |
27,59 |
28 |
28,9 |
0,864 |
|
|
Previous extensive |
17 |
29,31 |
20 |
20,6 |
0,219 |
|
|
Inferior |
23 |
60,34 |
45 |
46,4 |
0,413 |
|
|
Lower lateral |
0 |
0 |
2 |
2,06 |
0,271 |
|
|
Lateral |
1 |
1,72 |
2 |
2,06 |
0,883 |
|
|
Vessels responsible for infarction on admission (Coronary angiography) |
||||||
|
Anterior descending artery |
20 |
|
28 |
|
|
|
|
Right coronary artery |
12 |
|
29 |
|
|
|
|
Circumflex artery |
5 |
|
12 |
|
|
|
|
Left coronary trunk |
4 |
|
3 |
|
|
|
|
Number of vessels affected coronary angiography at admission |
||||||
|
No glass |
2 |
5,13 |
3 |
4,05 |
0,36651 |
|
|
One glass |
21 |
53,85 |
41 |
55,41 |
|
|
|
Two glasses |
13 |
33,33 |
16 |
21,62 |
|
|
|
Three glasses |
3 |
7,69 |
10 |
13,51 |
|
|
|
Four glasses |
0 |
0 |
4 |
5,41 |
|
|
|
Complications |
|
|||||
|
Deceased |
8 |
13,79 |
15 |
15,46 |
0,0516 |
|
|
Atrial fibrillation |
2 |
3,45 |
0 |
0 |
0,0657 |
|
|
Heart failure |
13 |
22,41 |
26 |
26,8 |
0,5421 |
|
The number of affected vessels for each patient was identified during the coronary angiography procedure. The evaluation of the extent of disease in the 113 coronary angiographies showed that most patients had one affected vessel, followed by two and three, respectively. Similar behavior was found in the analysis in both sexes.
Three complications were detected in the patients who attended. Heart failure was the most frequent, followed by death.
Of the 155 cases treated, 23 patients died. Of the total number of male patients, 15 % died, and 13 % of the total number of female patients. However, there were no significant differences in complications; a different behavior was observed in women regarding atrial fibrillation, which alerts to the need for follow-up of women in the event of the appearance of this type of arrhythmia.
Specifically, when death was related to the location of the infarction (table 2), it was observed that, of the 37 cases with extensive anterior location, 20 died (54,05 %, p=0,0000). This means that in this sample, patients with this location had a statistically high probability of death. This fact should be seen in women, who presented a higher frequency of extensive anterior AMI.
|
Table 2. Relationship between ST-elevation AMI location and mortality |
||||||
|
Location of myocardial infarction |
Deceased |
Alive |
Total |
p-value |
||
|
No. |
% |
No. |
% |
|||
|
Previous |
1 |
2,27 |
43 |
97,73 |
44 |
0,0056 |
|
Previous extensive |
20 |
54,05 |
17 |
45,95 |
37 |
0,0000 |
|
Inferior |
2 |
2,94 |
66 |
97,06 |
68 |
0,0002 |
|
Lower lateral |
0 |
0 |
2 |
100 |
2 |
0,5524 |
|
Lateral |
0 |
0 |
3 |
100 |
3 |
0,4653 |
Statistical analysis by sex showed that of the 20 men who had an ST-segment elevation AMI with extensive anterior topography, 12 died, for 60 %. Of the 15 men who died, extensive anterior topography was 80 %, p=0,0000. Eight of the 17 women with this topography died (47,1 %). Of the deceased women, 100 % had extensive anterior topography, p=0,0000.
In this study, the previous extensive topography was related to the high number of deaths in general and for each sex. All of the deceased females had this location.
DISCUSSION
Age as a risk factor for cardiovascular disease has been extensively studied, as has sex. It is universally known that the proportion of patients with ischemic heart disease is higher in the male sex; however, in menopausal women, this difference disappears. In support of this approach, it is pointed out that after 66 years of age, women are more diabetic, more obese, and more hypertensive due to the loss of estrogenic protection that they had at premenopausal ages.(7,8)
With age, there is a change in the pattern of risk factors in patients. As the influence of family history decreases, the frequency of smoking and hypercholesterolemia becomes more critical, as well as HT and diabetes mellitus.(8)
Several studies coincide with the predominance of the male sex in patients with AMI.(7,8) In Cuban patients(7,8), the most represented age groups were those between 60 and 79 years of age, which agrees with that reported by Morán Salinas(9) in patients from Paraguay.
Martínez Carrillo(10) showed similar results in his own Institute of Cardiology and Cardiovascular Surgery, in a sample of 431 patients over four years. The male patients had an average age of 61,96 ± 1,37 years, which was significantly lower (p = 0,000004) than that of the female patients (68,35 ± 2,42 years).
Similar data were obtained by Chávez et al.(11) in a Peruvian multicenter prospective study, with mean ages of 73,6 and 62,5 years in women and men, respectively, with significant differences. These statistics agree with the results of the present investigation.
Coronary risk factors are those that have demonstrated a strong and independent epidemiological association with coronary heart disease. The evolution of sex-specific research has shown that, although men and women share similar risk factors for coronary heart disease, some of them are more potent in women. Such as tobacco abuse.(5)
Linares(9) in patients showed significant differences between female diabetics and male diabetics. The excess proportion of infarcted females was also observed in the results of Chávez(11) and Morán Salinas(9), but similar to this research, the differences in proportions were insignificant.
Unhealthy alcohol consumption puts people’s health and safety at risk. Many people do not seek medical or psychological help because they do not recognize the problem they have, hence it is not always reported as history during a medical interview, even more so if it is explained to the patient that it can cause increased blood pressure, risk of cardiomegaly, heart failure and cerebrovascular disease, even that, with excessive consumption, atrial fibrillation may appear.(12)
In the clinical evaluation analysis, at admission, through the Killip Kimball, a lower number of cases without heart failure were observed (73,2 %), which may be determined by multiple factors, such as early and timely attention of patients with precordial pain and increased sensitivity in the diagnosis of AMI without heart failure. Like Chávez(11), women were more represented in classification III than men.
About the location of the infarction in a study of 396 patients with ST-segment elevation AMI, in contrast to this work, they found that the most frequent location in women was on the inferior aspect in more than half of the cases, followed by the anterior and lateral location; in contrast to men, where the most frequent location was anterior (in three-fifths of the patients), then inferior and finally lateral.(12)
When analyzing the vessels responsible for the infarction, the most affected artery, both in men and women, in a study carried out in 2020 in Havana, was the heart’s anterior descending or main artery, with 59,6 % of male cases.(13)
Another study from the National Hospital of Costa Rica found the right coronary and anterior descending arteries responsible in 39,5 % of the sample, the circumflex 14 %, and the left common trunk 2 %, in one case.(14)
About coronary artery involvement, the anterior descending artery was the most affected vessel in AMI, both of embolic and atherosclerotic origin, and it is confirmed that in an autopsy, coronary embolisms occur up to four times more frequently in the anterior descending artery than in the right coronary artery and circumflex artery.(15)
In a recent systematic review that included 129 clinical cases and case series of coronary embolisms, Lacey et al.(16) confirmed that the anterior descending artery was the most affected vessel (45,3 %). However, such differences in the distribution of culprit coronary vessels could be explained by the bias associated with the fact that arteries with larger territories are more likely to be autopsied.
The number of vessels affected was shown in a study conducted in Santiago de Cuba in which coronary angiography of 63 patients showed that 24 cases (38,1 %) had only one vessel affected; 19 patients (30,2 %) had 2-vessel disease, and 15 patients (23,8 %) had multivessel disease.(17)
In another characterization of the results of interventional procedures in patients with ST-segment elevation AMI, it was found that 53,9 % had one vessel affected, 14,3 % had two vessels, 4,6 % had three vessels, and 27,2 % had no lesions.(18)
When analyzing complications, Chávez et al.(11) showed a statistically significant excess of female deaths compared to male deaths.
There is scientific evidence of the differences in the form of presentation of this entity according to sex. The factors that contribute to the worse clinical evolution of women are: older age, greater frequency of comorbidities, and several underlying complications. Women usually have less significant acute coronary artery disease, but more frequently present with heart failure despite having better left ventricular function. A descriptive study of 138 patients in Granma describes that 51 patients presented complications, among which heart failure and atrial fibrillation stand out.(8)
Left ventricular dysfunction is the strongest independent predictor of mortality after this type of infarction. The degree of heart failure after myocardial infarction can be classified according to the Killip class: class I, absence of rales or third heart sound; class II, pulmonary congestion with rales extending < 50 % of the lung fields, sinus tachycardia or third heart sound; class III, pulmonary edema with rales extending > 50 % of the lung fields, and class IV, cardiogenic shock.(5)
Women are more likely to develop symptoms of heart failure in the context of AMI. It is proposed that women have a higher Killip class in the presentation of AMI (8), which did not coincide with this work.
Arrhythmias and conduction disturbances are frequent in the first hours after myocardial infarction. The incidence is 28 % for new-onset atrial fibrillations, 13 % for nonsustained ventricular tachycardia, 10 % for high-grade atrioventricular block, 7 % for sinus bradycardia, 5 % for sinus arrest, 3 % for sustained ventricular tachycardia, and 3 % for ventricular fibrillation.(5)
Women and men appear to be at similar risk for the development of ventricular arrhythmias after AMI. However, women are less likely to receive an Automatic Implantable Defibrillator for the primary or secondary prevention of Sudden Cardiac Death compared to men.(10)
Women and older patients are at increased risk of developing atrial fibrillation and are at increased risk of high-grade atrioventricular block in the setting of AMI.(12) In this case, only two patients had atrial fibrillation, and they were female.
In a study developed in Cuba in reperfused patients, it was found that the most frequent complications were: arrhythmia (10,8 %), cardiorespiratory arrest (9 %), which differ significantly from the others (p<0,05 in X2) such as shock (4,7 %) and death (4,4 %), among others.(10)
ST-elevation AMI is associated with a poor prognosis and a high incidence of death and cardiovascular events, especially those located in the anterior wall.(19) The results of the present investigation coincide with studies such as that of Ferrante et al.(20) who reported a high mortality rate in patients with anterior ST-elevation AMI, both in the short- and long-term follow-up.
Several recent studies have highlighted a decrease in acute and long-term mortality after ST-segment elevation AMI, in parallel with the increase in reperfusion therapy, primary percutaneous coronary intervention, modern antithrombotic treatment, and secondary prevention treatments.(13,15,16)
Despite this, mortality remains significant, justifying continued efforts to improve quality of care, adherence to guidelines and research.
CONCLUSIONS
1. The study shows that there are differences between men and women in terms of age and risk factors; men became ill at a younger age and smoking was the predominant known cardiovascular risk factor in this sex. The risk of cardiogenic shock was minimally higher in the male sex.
2. The clinical characteristics of infarction differed according to sex, the predominance of the descending anterior descending artery as the culprit artery and the involvement of two vessels make it necessary to pay close attention in health care settings to improve the early identification and management of women with ST-segment elevation myocardial infarction.
3. Women were more likely to present extensive anterior infarction, a topography that had a higher incidence of mortality as a complication, a useful finding for personalizing the care and treatment of ST-segment elevation acute myocardial infarction according to the sex of the patient.
REFERENCES
1. Lawton JS, Tamis-Holland JE, Bangalore S, y otros: 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 79 (2): e21–e129, 2022. doi: 10.1016/j.jacc.2021.09.006. Disponible en: https://www.ahajournals.org/doi/full/10.1161/ CIR.0000000000001039?rfr_dat=cr_pub+ +0pubmed&url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org
2. Tamis-Holland JE, Jneid H, Reynolds HR, y otros: Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease: A scientific statement from the American Heart Association. Circulation 139: e891–e908, 2019. doi: 10.1161/CIR.0000000000000670. Disponible en: https://www.ahajournals.org/doi/10.1161/ CIR.0000000000000670? url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
3. Cuba. Centro Nacional de Información de Ciencias Médicas. Biblioteca Médica Nacional. Cardiopatías y sexo. Bibliomed [Internet]. 2017 Ene [citado 2 FEB 2017];24(1): [aprox. 13 p.]. Disponible en: http://files.sld.cu/bmn/files/2016/12/bibliomed-enero-2017.pdf
4. Chandrashekhar Y, Narula J. Resource and Infrastructure-Appropriate Management of ST-Segment Elevation Myocardial Infarction in Low- and Middle-Income Countries. Circulation. 2020;141(1):2004-25. Disponible en: https://www.ahajournals.org/doi/10.1161/ CIRCULATIONAHA.119.041297? url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
5. Valladares-Carvajal F, Hernández-de-León N, Pérez-Alfonso C, León-Valdés G, Torres-Acosta C. Infarto agudo de miocardio con elevación del segmento ST. Guía de Práctica Clínica. Revista Finlay [revista en Internet]. 2022 [citado 2023 Mar 31]; 12(3): [aprox. 22 p.]. Disponible en: https://revfinlay.sld.cu/index.php/finlay/article/view/1024
6. Panting JR, Gatehouse PD, Yang GZ, Grothues F, Firmin DN,Collins P y otros. Abnormal subendocardial perfusion in cardiac syndrome X detected by cardiovascular magnetic resonance imaging. N Engl J Med [Internet]. 2002 Jun [cited 2017 May 5]; 346:1948-53. Available factores de riesgoom: http://www.nejm.org/doi/full/10.1056/NEJMoa012369#t=article.
7. Linares-Cánovas LP, Vilaú-Jiménez M, Vitón-Castillo AA, Linares-Cánovas LB. Caracterización de pacientes con IAM con elevación del segmento ST. Revista Electrónica Dr. Zoilo E. Marinello Vidaurreta. 2019; 44(2). Disponible en: http://revzoilomarinello.sld.cu/index.php/zmv/article/view/1511
8. Enamorado A, Goro G, García Cañete I, González M. Caracterización clínica y epidemiológica de pacientes con IAM con elevación del segmento ST. Rev Panorama. Cuba y Salud [Internet]. 2020 [citado]; 15(3):26-31. Disponible en: http:// www.revpanorama.sld.cu/index.php/rpan/article/view/
9. Morán Salinas Alberto Javier, Duarte Fariña Rubén Fernando, Ortiz Galeano Ignacio. Frecuencia de factores de riesgo coronarios en pacientes con IAM en el Servicio de Cardiología del Hospital de Clínicas. Rev. virtual Soc. Parag. Med. Int. [Internet]. 2019 Sep [cited 2023 Apr 14] ; 6( 2 ): 57-63. Available from: https://doi.org/10.18004/rvspmi/2312-3893/2019.06.02.57-063
10. Martínez-Carrillo A, Sainz---González-de-la-Peña B, Ramos-Gutiérrez B, Pacheco-Alvarez E, Zorio-Suarez B, Castañeda-Rodríguez G. Infarto agudo del miocardio con elevación del ST en el servicio de urgencias del Instituto de Cardiología. Revista Cubana de Cardiología y Cirugía Cardiovascular [Internet]. 2017 [citado 20 Abr 2023]; 23 (1):[aprox. 9 p.]. Disponible en: https://revcardiologia.sld.cu/index.php/revcardiologia/article/view/677
11. Chávez F, Espinola S, Chacón M. Diferencias relacionadas al Sexo en pacientes con IAM ST elevado. Arch Peru Cardiol Cir Cardiovasc [nternet]. 4 de mayo de 2020 [citado 14 de abril de 2023];1(1):31-6. isponible en: https://apcyccv.org.pe/index.php/apccc/article/view/10
12. Wittich, Christopher M. Mayo Clinic Internal Medicine Board Review. Oxford University Press, USA, 2019.
13. Sellén Sanchén Elizabeth, Hernández Valdés Enmanuel, Sellén Crombet Joaquín, Ybargollín Rosendo. Gender differences in the clinical and angiographic presentation of Acute Coronary Syndrome. Rev haban cienc méd [Internet]. 2020 Abr [citado 2023 Abr 14] ; 19( 2 ): e2918. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1729-519X2020000200003&lng=es. Epub 22-Abr-2020.
14. Acuna-Roman, Andrés; Vindas-Villarreal, Manuel Antonio, Salas-Segura, Donato A.. Perfil clínico y angiográfico de las mujeres con infarto agudo al miocardio en un hospital nacional. Acta méd. costarric [online]. 2021, vol.63, n.2 [cited 2023-04-15], pp.97-103. Available from: http://www.scielo.sa.cr/scielo.php?script=sci_arttext&pid=S0001-60022021000200097&lng=en&nrm=iso. ISSN 0001-6002
15. Baza, Adrián Jerónimo, et al. “Predictores clínicos y características angiográficas del infarto agudo de miocardio por embolia sistémica.” REC: Interventional Cardiology 4.4 2022: 287-293.
16. Lacey MJ, Raza S, Rehman H, Puri R, Bhatt DL, Kalra A. Coronary embolism: A systematic review. Cardiovasc Revasc Med. 2020; 21:367-374. Disponible en:
17. Torres MR, ; Peña S ; García, E: Caracterización del IAM en pacientes entre 45 y 59 años de edad. Revista Cubana de Cardiología y Cirugía Cardiovascular, ISSN-e 1561-2937, Vol. 25, Nº. 4, 2019 (Ejemplar dedicado a: Oct-Dic), págs. 548-559.
18. Fabré, A. S., Querol, N. A. S., Amiot, T. C., Guevara, Y. G., Pacheco, I. A. C. S., & Oliva, A. R.. Intervencionismo Coronario Percutáneo en pacientes con IAM menores de 50 años. In Cuba Salud, 2022, May.
19. Yi-ming Li, Li-cheng Jiang, Jing-jing He, Kai-yu Jia, Yong Peng, Mao Chen. Machine Learning to Predict the 1-Year Mortality Rate After Acute Anterior Myocardial Infarction in Chinese Patients, Therapeutics and Clinical Risk Management, 2020, 16: 1-6, disponible en: https://www.tandfonline.com/doi/full/10.2147/TCRM.S236498
20. Ferrante, G.; Barbieri, L.; Sponzilli, C.; Lucreziotti, S.; Salerno Uriarte, D.; Centola, M. y otros. Predictors of Mortality and Long-Term Outcome in Patients with Anterior STEMI: Results from a Single Center Study. J. Clin. Med. 2021, 10, 5634. https://doi.org/10.3390/jcm10235634
FUNDING
None
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHOR CONTRIBUTION
Conceptualization: Anabel Sánchez Orraca, Miladys Orraca Castillo, Damaris Hernández Véliz.
Data curation: Anabel Sánchez Orraca, Miladys Orraca Castillo, Damaris Hernández Véliz.
Formal analysis: Anabel Sánchez Orraca, Miladys Orraca Castillo, Damaris Hernández Véliz.
Research: Anabel Sánchez Orraca, Miladys Orraca Castillo, Damaris Hernández Véliz.
Methodology: Anabel Sánchez Orraca, Miladys Orraca Castillo, Damaris Hernández Véliz.
Project management: Anabel Sánchez Orraca, Miladys Orraca Castillo, Damaris Hernández Véliz.
Resources: Anabel Sánchez Orraca, Miladys Orraca Castillo, Damaris Hernández Véliz.
Software: Anabel Sánchez Orraca, Miladys Orraca Castillo, Damaris Hernández Véliz.
Supervision: Anabel Sánchez Orraca, Miladys Orraca Castillo, Damaris Hernández Véliz.
Validation: Anabel Sánchez Orraca, Miladys Orraca Castillo, Damaris Hernández Véliz.
Visualization: Anabel Sánchez Orraca, Miladys Orraca Castillo, Damaris Hernández Véliz.
Writing – original draft: Anabel Sánchez Orraca, Miladys Orraca Castillo, Damaris Hernández Véliz.
Writing – review and editing: Anabel Sánchez Orraca, Miladys Orraca Castillo, Damaris Hernández Véliz.