doi: 10.62486/agmu202468
ORIGINAL
Magnetic resonance imaging findings in cervical pathologies and its’ correlation with patient´s body mass index in Anambra state, Nigeria: a cross-sectional study
Hallazgos de resonancia magnética en patologías cervicales y su correlación con el índice de masa corporal del paciente en el estado de Anambra, Nigeria: estudio transversal
Michael Promise Ogolodom1
![]() *, Chukwuma Martha Chinazo2, Anelechi Kenneth Madume3,
Olukumnmi Ijeruh4, Abdul Fatai K. Bakre5, Nwamaka Chizube
Ikegwuonu6, Emeka Emmanuel Ezugwu2, Abam Rufus4,
Nengi Alazigha4, Egop Brownson Egop7, Christian
Maduabuchi Eke8
*, Chukwuma Martha Chinazo2, Anelechi Kenneth Madume3,
Olukumnmi Ijeruh4, Abdul Fatai K. Bakre5, Nwamaka Chizube
Ikegwuonu6, Emeka Emmanuel Ezugwu2, Abam Rufus4,
Nengi Alazigha4, Egop Brownson Egop7, Christian
Maduabuchi Eke8
1Department of Radiography, Faculty of Basic Medical Sciences, Rivers State University. Port Harcourt, Nigeria.
2Department of Radiography and Radiological Sciences, Nnamdi Azikiwe University, Nnewi Campus. Anambra State, Nigeria.
3Department of Physiotherapy, Faculty of Basic Medical Sciences, College of Medical Sciences, Rivers State University. Port Harcourt, Nigeria.
4Department of Radiology, Rivers State University Teaching Hospital. Port Harcourt, Nigeria.
5Department of Radiography and Radiation Sciences, Faculty of Basic Medical Sciences, Osun State University. Oshogbo, Nigeria.
6Department of Radiology, Nnamdi Azikiwe University Teaching Hospital. Nnewi, Anambra State, Nigeria
7Department of Radiology, Rivers State Government House Clinics. Port Harcourt, Nigeria
8Department of Radiography and Radiation Sciences, Faculty of Allied Health Sciences, Gregory University. Uturu, Abia State, Nigeria.
Cite as: Ogolodom MP, Brownson Egop E, Alazigha N, Rufus A, Ezugwu EE, Ikegwuonu NC, et al. Magnetic resonance imaging findings in cervical pathologies and its’ correlation with patient´s body mass index in Anambra state, Nigeria: a cross-sectional study. Multidisciplinar (Montevideo). 2024; 2:68. https://doi.org/10.62486/agmu202468
Submitted: 27-11-2023 Revised: 22-03-2024 Accepted: 30-08-2024 Published: 31-08-2024
Editor:
Telmo
Raúl Aveiro-Róbalo ![]()
Corresponding Author: Michael Promise Ogolodom *
ABSTRACT
Introduction: subsequent to the multitude of cervical pathologies with aging, this study aims to determine the prevalence and pattern of magnetic resonance imaging (MRI) cervical pathologies and its correlation with body mass index (BMI).
Methods: a cross-sectional retrospective study was conducted in some selected diagnostic centres in Anambra State, Nigeria using 141 MRI data that met the inclusion criteria. Data were collected from patients` request cards, MRI screening form and MRI scan reports. Both descriptive and inferential (Pearson`s correlation test) were used as tools for statistical analysis. The level of significance was set at the level of less than 0,05.
Results: out of the 141 sample size, the majority 93 (66 %) were males while females accounted for 48 (34 %). The greater number 36 (25,4 %) of patients were within the age range of 61-70years of age. Greater number 83 had normal BMI (18,5-<25) and the least 3 were underweight (<18,5), 50 were overweight (25-<30) and 5 were obese (>30).Out of the 141 patients, most 68 (48,2 %) had single pathology, 51 (36,2 %) had double pathologies and few patients 22 (15,6 %) had multiple pathologies. There was a negative correlation between pathology and BMI that is not statistically significant(r= -0,04, p = 0,63). Also, there was negative correlations between patterns of spinal involvement and BMI, which is not statistically significant ( r= -0,130, p = 0,126).
Conclusion: there is prevalence of cervical pathologies mostly in males in their 6th decade and the 4th decade with more of single pattern pathologies. The common level of involvement is at C5 vertebra. Intervertebral osteochondrosis and spondylosis was found to be the commonest cervical pathology among the study population. However, there was no statistically significant correlation between cervical pathologies and its pattern of occurrence with body mass index.
Keywords: Cervical; Body Mass Index; Disease; Magnetic Resonance Imaging; Obesity.
RESUMEN
Introducción: a raíz de la multitud de patologías cervicales con el envejecimiento, este estudio pretende determinar la prevalencia y el patrón de patologías cervicales por resonancia magnética (RM) y su correlación con el índice de masa corporal (IMC).
Métodos: se realizó un estudio retrospectivo transversal en algunos centros de diagnóstico seleccionados del estado de Anambra, Nigeria, utilizando 141 datos de RM que cumplían los criterios de inclusión. Los datos se recopilaron a partir de las tarjetas de solicitud de los pacientes, el formulario de cribado de IRM y los informes de las IRM. Para el análisis estadístico se utilizaron herramientas descriptivas e inferenciales (prueba de correlación de Pearson). El nivel de significación se fijó en menos de 0,05.
Resultados: de una muestra de 141 personas, la mayoría, 93 (66 %), eran varones, mientras que las mujeresrepresentaban 48 (34 %). El mayor número de pacientes, 36 (25,4 %), tenía entre 61 y 70 años. El mayor número, 83, tenía un IMC normal (18,5-<25) y el menor, 3, bajo peso (<18,5), 50, sobrepeso (25-<30) y 5, obesidad (>30). De los 141 pacientes, la mayoría, 68 (48,2 %), tenía una sola patología, 51 (36,2 %), dos patologías y unos pocos, 22 (15,6 %), tenían patologías múltiples. Existe una correlación negativa entre la patología y el IMC que no es estadísticamente significativa (r= -0,04, p = 0,63). También se observó una correlación negativa entre los patrones de afectación de la columna vertebral y el IMC, que no es estadísticamente significativa ( r= -0,130, p = 0,126).
Conclusiones: existe prevalencia de patologías cervicales mayoritariamente en varones en su 6ª década y en la 4ª década con más de patologías de patrón único. El nivel común de afectación es la vértebra C5. La osteocondrosis intervertebral y la espondilosis resultaron ser las patologías cervicales más frecuentes entre la población estudiada. Sin embargo, no hubo correlación estadísticamente significativa entre las patologías cervicales y su patrón de aparición con el índice de masa corporal.
Palabras clave: Cervical; Índice de Masa Corporal; Patología; Resonancia Magnética; Obesidad.
INTRODUCTION
There is a multitude of pathologies affecting the cervical spines and their prevalence is increasing with the aging population.(1) The spectrum of cervical spine pathologies includes degenerative, traumatic, infectious, neoplastic, congenital, inflammatory, autoimmune, and vascular pathologies.(2) The most common of these pathologies is spondylosis which is a degenerative process of the spine with a gradual onset. Alone or in combination with other factors, it causes spinal cord compression and canals stenosis.(3)
According to Ogolodom et al.(1), imaging of the spine has a very important role in the diagnosis and treatment of cervical spine disorders. The modalities for the imaging and assessment of spinal pathologies includes; conventional radiography, computed tomography (CT) and magnetic resonance imaging (MRI). Currently, magnetic resonance imaging (MRI) is the modality of choice for diagnosis of pathologies and other abnormalities related to the spinal column and the intervertebral disc when compared with plain radiography and computed tomography, either separately or combined.(4) The sensitivity of T1 and T2 weighted magnetic resonance imaging (MRI) is almost 100 %, it gives detailed information about the intervertebral discs, intervertebral foramina, vertebrae, facets, joints and ligaments especially on sagittal plane images. It is also a non-invasive procedure.(5)
Increasing body mass index (BMI) which may progress to obesity is a growing public health concern globally and the number of overweight or obese individuals is dramatically increasing worldwide.(6) The global epidemic of overweight and obesity- “globesity” - is rapidly becoming a major public health problem in many parts of the world.
The latest figures from the World Health Organization(7) showed that worldwide obesity has nearly tripled since 1975. In 2016, 650 million (13 %) and 1,9 billion (39 %) of the world adult population were obese and overweight respectively. It has been projected that many European countries will have an obesity prevalence of 20 % to 43 % by 2025(8) and that by 2030, 51 % of the American population will be obese.(9) In Nigeria, Chukwunonye et al.(10) undertook a systematic review of four articles published from January 2001 to September 2012 on the prevalence of overweight and obesity in adult Nigerians and found that the prevalence of overweight ranged from 20,3 % to 35,1 %, while the prevalence of obesity ranged from 8,1 % to 22,2 %.
Increased BMI leads to increased load bearing and it has also been suggested that metabolic factors associated with obesity may be detrimental to healthy vertebral column.(11) The body mass index is used to broadly categorize a person as underweight, normal weight, overweight, or obese based on tissue mass (muscle, fat, and bone) and height. Major adult body mass index classifications are underweight (under 18,5 kg/m2), normal weight (18,5 to 24,9), overweight (25 to 29,9), and obese (30 or more).
Similar studies have been conducted such as the impact of body mass index on severity of cervical spine fracture by Choo et al.(12), which concluded that patients with higher BMI may be predisposed to more severe cervical spine fracture and/or SCI(spinal cord injury) after MVA(motor vehicle accident), especially when rollover is present. Another similar study by Sheng et al.(13) concluded that there is a positive correlation between BMI and spinal injuries.
Considering the increasing risk of many diseases, which associated with increased BMI, it would be necessary to determine if there exist any correlations between cervical spine pathologies diagnosed on MRI and BMI among those residing in Anambra State. To the best of our knowledge, this has not been assessed. Therefore, this study was designed to evaluate the MRI findings in cervical spine pathologies and its correlations with the body mass index in some selected diagnostic centres in Anambra State, Nigeria.
METHOD
This was a retrospective cross-sectional study conducted with 141 patients’ MRI data at some selected diagnostic centres in Anambra State, Nigeria from November 2023 to December, 2023. The 141 patients’ MRI data was determined using the Taro Yamane formula cited by Ukaji et al.(14) study and were selected purposively based on the inclusion criteria of data with diagnosed cases of cervical pathologies, present of recorded height and weight of the patient and demographic variables such as age and gender. The ethical approval (NAU/FHST/2023/RAD/01) for the study was obtained from the Human Resource Ethics Committee of the Faculty of Health Science and Technology, College of Health Sciences, Nnewi Campus, Nnamdi Azikiwe University. The purpose of the study was adequately explained to the management of the selected facilities that was used for this study. Every data that was collected was kept in strict confidence and used only for the sole purpose of this research.
Data were collected from secondary source. The data that was collected includes:
1. Data from request cards and MRI screening form including:
i. Patient’s age.
ii. Patient’s sex.
iii. Clinical history.
iv. Patient’s height and weight.
2. Data from MRI scan reports including:
i. MRI imaging findings.
ii. Patient weight and date of the examination.
iii. Information gathered from the Radiologists’ reports included definitive findings as shown in MRI scan images.
The above data were collected using data capture sheet designed for the purpose of this study. The obtained data were categorized according to the study objectives and subjected to statistical package for social sciences (SPSS) version 21. Both descriptive (mean, frequency, percentage, bar chart) and inferential (Pearson’s correlation test) statistics were used as tool for statistical analysis. The level of significance was set at p-value less than 0,05.
RESULTS
Out of the 141 sample size, the majority 93 (66 %) were males while females accounted for 48 (34 %) (figure 1). The greater number 36 (25,4 %) of patients were within the age range of 61-70years of age while the least number 2 (1,4 %) were within the age group 10-20 years as presented in figure 2. Their age ranges from19-81 years with a mean age of 52,7 years (figure 2). Greater number 83 had normal BMI (18,5-<25) and the least 3 were underweight (<18,5), 50 were overweight (25-<30) and 5 were obese (>30) (table 1).Out of the 141 patients, most 68 (48,2 %) had single pathologies, 51 (36,2 %) had double pathologies and few patients 22 (15,6 %) had multiple pathologies. Among the single pathologies, intervertebral osteochondrosis occurred most 11 (7,8 %) followed by cervical spondylosis 9 (6,4 %) (table 2a). From the double pathologies’ category, cervical osteochondrosis and compressive myelopathy occurred most 13 (9,1 %) followed by cervical spondylosis and spinal canal stenosis 5 (3,5 %) (table 2b). In the multiple pathologies group, cervical spondylosis, intervertebral disc dessication and bulging have the same number of occurrences 2 (1,4 %) with intervertebral Osteochondrosis, spinal canal stenosis, neural foramina narrowing as seen in table 2c.As presented in table 3, in the single pathology group, the most 8 (5,6 %) level of involvement of the cervical spine is at C5 followed by C6 6 (4,2 %), C7 5 (3,5 %) and C4 (2,1 %). There is no single pathology in C1, C2 and C3. In the double pathologies’ category, C5 and C6 were mostly affected 19 (13,3 %) each respectively followed by C4, C5 and C6, C7 in which 9 (6,3 %) patients each were affected at this level. Only 9 (6,3 %) patients in the multiple pathologies group were mostly affected at C4, C5, C6 level followed by C4, C5, C6, C7 in which 6 (4,2 %) patients each were affected.) The result in table 4 revealed negative correlations between pathology and BMI that is not statistically significant(r= -0,04, p = 0,63). From table 5, there was negative correlations between patterns of spinal involvement and BMI, which is not statistically significant( r= -0,130, p = 0,126).
Figure 1. Bar chart showing frequency and percentage of gender
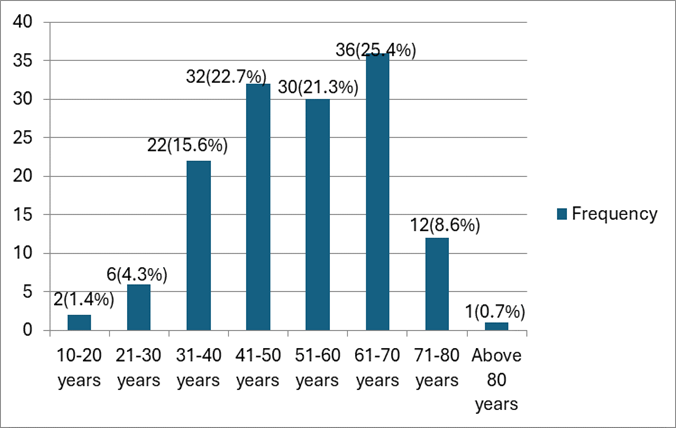
Figure 2. Bar chart showing frequency and percentage of Age group
|
Table 1. BMI ranges and pattern of spinal involvement |
||||
|
BMI groups |
Pattern |
Frequency |
Percent |
|
|
<18,5 |
|
Double pattern |
1 |
33,3 |
|
Multiple pattern |
2 |
66,7 |
||
|
18,5 to < 25 |
|
Single pattern |
11 |
13,3 |
|
Double pattern |
59 |
71,1 |
||
|
Multiple pattern |
13 |
15,7 |
||
|
25 to < 30 |
|
Single pattern |
9 |
18,0 |
|
Double pattern |
32 |
64,0 |
||
|
Multiple pattern |
9 |
18,0 |
||
|
30 and above |
|
Single pattern |
3 |
60,0 |
|
Double pattern |
1 |
20,0 |
||
|
Multi pattern |
1 |
20,0 |
||
|
Total |
|
|
141 |
100 |
|
Table 2a. Frequency and percentage distribution of cervical Spine pathologies |
||
|
Cervical pathologies |
Frequency |
Percentage |
|
Single Pathology |
|
|
|
Background cervical Spondylosis |
1 |
0,7 |
|
Burst fracture |
4 |
2,8 |
|
C4 anterior tear drop fracture |
1 |
0,7 |
|
C4 anterior tear drop fracture Burst of B5 |
1 |
0,7 |
|
Cervical spine mass |
1 |
0,7 |
|
Compressive myelomalacia |
2 |
1,4 |
|
Disc degeneration |
1 |
0,7 |
|
Early cervical spondylodiscal disease |
2 |
1,4 |
|
Early intervertebral osteochondrosis |
5 |
3,5 |
|
Early onset of disc dessication |
2 |
1,4 |
|
Intervertebral disc desiccation |
4 |
2,8 |
|
Intervertebral disc disruption |
3 |
2,1 |
|
Intervertebral osteochondrosis |
11 |
7,8 |
|
Intraspinal mass |
2 |
1,4 |
|
Mild spondylosis |
2 |
1,4 |
|
Myelopathy |
2 |
1,4 |
|
Paravertebral collection |
4 |
2,8 |
|
Radiculopathy |
2 |
1,4 |
|
Segmental spinal cord oedema |
4 |
2,8 |
|
Spinal cord compressive myelopathy |
1 |
0,7 |
|
Spinal metastasis |
1 |
0,7 |
|
Spinal stenosis |
1 |
0,7 |
|
Spondylodiscal disease |
2 |
1,4 |
|
Cervical Spondylosis Total |
9 68 |
6,4 48,2 |
|
Table 2b. Frequency and percentage distribution of cervical spine pathologies |
||
|
Cervical pathologies |
Frequency |
Percentage |
|
Double Pathology |
|
|
|
Anterior disc bulge, spondylosis |
1 |
0,7 |
|
Cervical osteochondrosis, Neuroforaminal compromise |
1 |
0,7 |
|
Cervical spondylosis Spinal canal stenosis |
3 |
2,1 |
|
Diffuse facet joint hypertrophy Spondylosis |
1 |
0,7 |
|
Foraminal narrowing, Myelopathy |
1 |
0,7 |
|
Foraminal narrowing, radiculopathy |
1 |
0,7 |
|
Intervertebral disc desiccation, Cervical spondylosis and bulging |
1 |
0,7 |
|
Intervertebral disc desiccation, Scoliosis |
1 |
0,7 |
|
Moderate disc dessication, Spinal canal narrowing |
1 |
0,7 |
|
Intervertebral Osteochondrosis with neuroforamina narrowing |
1 |
0,7 |
|
Intervertebral Osteochondrosis, Compressive myelopathy |
13 |
9,1 |
|
Intervertebral Osteochondrosis, Diffuse facet joint hypertrophy |
1 |
0,7 |
|
Paraspinal hematoma, Spinal cord compressive myelopathy |
2 |
1,4 |
|
Paraspinal hematoma, Myelopathy |
1 |
0,7 |
|
Posterior disc bulge, Scoliosis |
1 |
0,7 |
|
Posterior disc bulge, Spondylosis |
1 |
0,7 |
|
Posterior disc protrusion and spinal stenosis |
2 |
1,4 |
|
Radiculopathy, Spondylosis |
1 |
0,7 |
|
Scoliosis, Intervertebral disc dessication |
2 |
1,4 |
|
Scoliosis, Posterior disc bulge |
1 |
0,7 |
|
Spinal canal stenosis, Cervical spondylosis |
5 |
3,5 |
|
Spondylolisthesis, Myelopathy |
1 |
0,7 |
|
Spondylosis with radiculopathy |
1 |
0,7 |
|
Spondylosis, Compressive myelopathy |
2 |
1,4 |
|
Spondylosis, Diffuse facet joint hypertrophy |
1 |
0,7 |
|
Spondylosis, Multi level posterior disc bulges |
1 |
0,7 |
|
Spondylolisthesis, Myelopathy |
1 |
0,7 |
|
Vertebral and spinal cord contusion Total |
2 51 |
1,4 36,2 |
|
Table 2c. Frequency and percentage distribution of cervical spine pathologies |
||
|
Cervical pathologies |
Frequency |
Percentage |
|
Multiple Pathology |
|
|
|
Cervical spondylosis, Intervertebral disc dessication and bulging |
2 |
1,4 |
|
Compression myelopathy, intervertebral Osteochondrosis |
1 |
0,7 |
|
Compressive myelopathy, Spondylosis, Spondylolisthesis ,spondylodiscitis and foramina narrowing |
1 |
0,7 |
|
myelopathy, spondylosis, Foraminal narrowing |
1 |
0,7 |
|
Compressive myelopathy, Spondylosis, spondylosis, Foramina narrowing |
1 |
0,7 |
|
Foramina narrowing, compressive myelopathy,spondylosis |
1 |
0,7 |
|
Foraminal narrowing,Myelopathy, secondary to posterior disc herniation |
1 |
0,7 |
|
Generalized endplate osteophytes, Multi-level posterior disc bulges |
1 |
0,7 |
|
Intervertebral disc desiccation, Cervical spondylosis and bulging |
1 |
0,7 |
|
Multi-level posterior disc bulges, Generalized endplate osteophytes |
1 |
0,7 |
|
Myelopathy, secondary to posterior disc herniation, foraminal narrowing |
1 |
0,7 |
|
Myelopathy,foraminal narrowing, Spinal stenosis |
1 |
0,7 |
|
Intervertebral Osteochondrosis, Spinal canal stenosis, Neural foramina narrowing |
2 |
1,4 |
|
Posterior disc bulge Cervical lordosis Grade 1 retro- listhesis, Grade 1 antero-listhesis |
1 |
0,7 |
|
Spinal canal stenosis, Foraminal, narrowing radiculopathy |
1 |
0,4 |
|
Spinal stenosis, Myelopathy,foraminal narrowing |
1 |
0,7 |
|
Spondylolisthesis, Moderate disc dessication, Spinal canal narrowing |
1 |
0,2 |
|
Spondylolisthesis, Posterior disc bulge, Cervical lordosis |
1 |
0,7 |
|
Spondylosis, Spondylolisthesis, Spondylodiscitis, foramina narrowing, Compressive myelopathy |
1 |
0,7 |
|
Spondylosis, Post disc protrusion, Spinal stenosis
Total |
1 22 141 |
0,7 15,6 100,0 |
|
Table 3. Frequency and percentage of spinal level of involvement |
||
|
Spinal levels |
Frequency |
Percent |
|
Single level |
|
|
|
C4 |
3 |
2,1 |
|
C5 |
8 |
5,6 |
|
C6 |
6 |
4,2 |
|
C7 |
5 |
3,5 |
|
Double |
|
|
|
C1,C5 |
1 |
0,7 |
|
C1,C7 |
1 |
0,7 |
|
C2,C3 |
2 |
1,4 |
|
C2,C5 |
1 |
0,7 |
|
C2,C6 |
2 |
1,4 |
|
C2,C7 |
1 |
0,7 |
|
C3,C4 |
8 |
5,6 |
|
C3,C5 |
6 |
4,2 |
|
C3,C6 |
5 |
3,5 |
|
C3,C7 |
7 |
4,9 |
|
C4,C5 |
9 |
6,3 |
|
C4,C6 |
6 |
4,2 |
|
C4,C7 |
6 |
4,2 |
|
C5,C6 |
19 |
13,3 |
|
C5,C7 |
7 |
4,9 |
|
C6,C7 |
9 |
6,3 |
|
Multiple |
|
|
|
C2,C3,C4 |
2 |
1,4 |
|
C2,C3,C4,C5 |
2 |
1,4 |
|
C3,C4,C5 |
2 |
1,4 |
|
C3,C4,C5,C6 |
1 |
0,7 |
|
C3,C5,C6 |
2 |
1,4 |
|
C4,C5,C6 |
9 |
6,3 |
|
C4,C5,C6,C7 |
6 |
4,2 |
|
C5,C6,C7 |
3 |
2,1 |
|
C6,C7,T1 |
2 |
1,4 |
|
Total |
141 |
100 |
|
Table 4. Correlation of Pathology and Body Mass Index |
||||
|
Variable |
N |
Correlation |
P-value |
Remark |
|
Pathology vs BMI |
141 |
-0,04 |
0,63 |
N/S |
|
Table 5. Correlation of patterns of spinal involvement and Body Mass Index |
||||
|
Variable |
N |
Correlation |
P-value |
Remark |
|
Disease patterns vs BMI |
141 |
-0,130 |
0,126 |
N/S |
|
Note: p>0,05= NS; P<0,05 = Sig. |
||||
DISCUSSION
This study findings revealed that majority of the patients with cervical pathologies were males. This is similar to the studies conducted by Ogolodom et al.(1), Choo et al.(12), Ogolodom, Ugwu et al.(15). However, Alghamdi et al.(16) found a higher frequency of females than males. The reason for higher male frequency in this study could be that males account for greater numbers of the workforce in our societies and are commonly exposed to spinal pathology predisposing factors such as strenuous jobs.
Cervical pathologies were most commonly found in patients within the 6th decade 36 (25,4 %) followed by the 4th decade 32 (22,7 %) and 5th decade 30 (21,3 %). This spike in cervical pathologies among patients within the 6th decade could be attributed to weakening and wearing of spine and its structures with age. The high frequency of cervical pathologies in the 4th decade could be attributed to the strenuous work done by people within this range as it is their active stage. The mean age of the patients was 52,7 years and the standard deviation is 14,2. the findings of the common age affected with cervical pathologies is inconsistent with findings of Ogolodom et al.(1), Choo et al.(12), Ogolodom et al.(15) and Alghamdi et al.(16). The difference could be attributed to the difference in the sample population used for the studies.
Intervertebral osteochondrosis which is a severe stage of spondylosis was the most common finding among single pathologies that had the highest frequency. This findings were similar to the findings of Ogolodom et al.(1,15) and Alghamdi et al.(16), but inconsistent with the results of Maaji et al.(17) and Karki et al.(18).
The prevalent level of cervical spine involvement in the single pathology category was at C5 which is consistent with studies of Ogolodom et al.(15) and Karki et al.(18). Similarly, Alghamdi et al.(16) and Matttei et al.(19) in their studies found the most common involvement to be the lower cervical regions(C5-C7) which Mattei et al.(19) attributed to the fact that the spinal cord accommodates three-quarters of the spinal canal at these levels and the vulnerable blood supply to this segment of the cord. However, Olarinoye-Akorede et al.(3) found the most common level of cervical pathologies to be C3, C4. The differences may be due to the sample characteristics and the context in which these studies were conducted.
We also found that there was a negative non-statistically significant correlation between pathologies and patterns of spinal involvements with body mass index. These findings imply that with respectively of the fact that BMI correlate with pathology and patterns of spinal involvement, it is in the reverse order and were not statistically noticeable. This could be attributed to sample size studied. These findings are not in agreement with the findings of the study conducted by Sheng et al.(13), which reported a positive correlation between BMI and spinal injuries. These differences could be due to differences in our sample sizes as well as the geographical variations of our studies.
CONCLUSIONS
There is prevalence of cervical pathologies mostly in males in their 6th decade and the 4th decade with more of single pattern pathologies. The common level of involvement is at C5 vertebra. Intervertebral osteochondrosis and spondylosis was found to be the commonest cervical pathology among the study population. However, there was no statistically significant correlation between cervical pathologies and its pattern of occurrence with body mass index.
BIBLIOGRAPHIC REFERENCES
1. Ogolodom MP, Ugwu AC, Akosile CO, Okpaleke MS, Mbaba AN, Eja-Egwu UN et al . Magnetic resonance imaging findings in cervical and lumbar pathologies and their impact on patients` quality of life. Afr. J. Health Sci. 2021 34(5): 681 – 694.
2. Chung A. Lumbar Spine (Lower Back) Anatomy and function. 2019. Healthpages.org. Available from: healthpages.org/anatomy-function/lumbar-spine-lower-back. Accessed on December 23, 2023.
3. Olarinoye – Akorede SA, Ibinaiye PO,Akano A, Hamidu AU and Kajogbola GA. Magnetic resonance imaging findings in cervical spondylosis and cervical spondylotic myelopathy in Zaria, Northern Nigeria, Sub-Saharan Afr J Med; 2015, 2(2): 74 – 78.
4. Chiu WT, Lin HC, Lam C, Chu S, Chiang Y, Tsai S. Review Paper: Epidemiology of Traumatic Spinal Cord Injury: Comparisons between developed and Developing Countries. Asia Pac J Public Health; 2020, 22:9-18.
5. Mustapha Z, Okedayo M, Ibrahim K, Abbs AA, Ahmadu MS, Abubaka et al. Cervical spine MRI findings in patients presenting with Neck pain and Radiculopathy. Inter ResJ Basic and Clin Stud; 2014,2(2): 20 –26.
6. Ugwu A. Relationship of the Body Mass Index (BMI) with the lumbar radiological findings in the incidences of low back pain. 2019, Afribary.com:Retrieved December 20, 2023, from https://afribary.com/works/relationship-of-the-body-mass-index-bmi-with-the-lumbar-radiological-findings-in-the-incidences-of-low-back-pain-4105
7. World Health Organization (2020) Obesity and Overweight Fact Sheet.
8. Pineda E, Sanchez-Romero LM, Brown M, Jaccard A, Jewell J, Galea G, Webber L, Breda J . Forecasting Future Trends in Obesity across Europe: The Value of Improving Surveillance. Obes Facts, 2018, 11(5):360-371.
9. Finkelstein E A, Khavjou O A, Thompson H , Trogdon J G, Pan L, Sherry B, Dietz W. Obesity and Severe Obesity Forecasts Through 2030. American Journal of Preventive Medicine, 2012, 42, (6):563-570.
10. Chukwuonye I.I, Chuku A, John C, Ohagwu K.A, Imo M.E, Isa S.E, Ogah O.S et al Prevalence of Overweight and Obesity in Adult Nigerians—A Systematic Review. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, 2013, 6, 43-47.
11. Hershkovich O, Friedlander A, Gordon B, Arzi H, Derazne E, Tzur D, et al .Associations of body mass index and body height with low backpain in 829,791 adolescents. Amer J Epidemiol; 2013, 178(4):603-609
12. Choo S, Jain N, Malik AT, Genneli T, Yu E .The impact of body mass index on severity of cervical spine fracture: A retrospective cohort study. J Craniovertebr Junction Spine, 2019, 10(4):224-228
13. Sheng B, Feng C, Zhang D, Splitler H, Shi L. Associations between obesity and spinal diseases: A medical expenditure panel study analysis. Int. J. Environ. Res. Public Health, 2017, 14,183.
14. Ukaji N F, Ohagwu CC, Ogolodom MP. Effects of Variations in Imaging Parameters on Image Quality of Non Contrast Computed Tomography Scans of Brain: A Cross-sectional Study. JCDR. 2021, 15(10):TC13-TC15
15. Ogolodom MP, Ugwu AC, Akosile CO. Magnetic resonance imaging findings and socio-demographic details of patients diagnosed with cervical spine pathologies in Rivers State. The South African Raiographers. 2022, 60.
16. Alghamdi A, Alqahtani A Magnetic Resonance Imaging of the Cervical Spine: Frequency of Abnormal Findings with Relation to Age Medicines, 2021: 8: 77.
17. Maaji SM, Saidu SA, Shamaki AMB, Danfulani M, Yunusa GH, Kakale SB. Spinal MRI findings in patients with signs and symptoms of radiculopathy in Sokoto, North-Western Nigeria. Kanem J Med Sci. 2012, 12(6):15-22
18. Karki DB, Panta OB, Gurung G. Non degenerative disease in MRI cervical spine of symptomatic patients. J Coll Med Sci Nepal. 2015, 11(4):20-23.
19. Mattei TA, Goulart CR, Milano JB, Dutra LPF, Fasset DR. Cervical spondylotic myelopathy: pathophysiology, diagnosis, and surgical techniques. ISRN Neurol. 2011:463729
FINANCING
The authors did not receive financing for the development of this research.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORSHIP CONTRIBUTION
Conceptualization: Michael Promise Ogolodom, Chukwuma Martha Chinazo, Anelechi Kenneth Madume, Olukumnmi Ijeruh, Abdul Fatai K. Bakre, Nwamaka Chizube Ikegwuonu, Emeka Emmanuel Ezugwu, Abam Rufus, Nengi Alazigha, Egop Brownson Egop, Christian Maduabuchi Eke.
Investigation: Michael Promise Ogolodom, Chukwuma Martha Chinazo, Anelechi Kenneth Madume, Olukumnmi Ijeruh, Abdul Fatai K. Bakre, Nwamaka Chizube Ikegwuonu, Emeka Emmanuel Ezugwu, Abam Rufus, Nengi Alazigha, Egop Brownson Egop, Christian Maduabuchi Eke.
Methodology: Michael Promise Ogolodom, Chukwuma Martha Chinazo, Anelechi Kenneth Madume, Olukumnmi Ijeruh, Abdul Fatai K. Bakre, Nwamaka Chizube Ikegwuonu, Emeka Emmanuel Ezugwu, Abam Rufus, Nengi Alazigha, Egop Brownson Egop, Christian Maduabuchi Eke.
Drafting - original draft: Michael Promise Ogolodom, Chukwuma Martha Chinazo, Anelechi Kenneth Madume, Olukumnmi Ijeruh, Abdul Fatai K. Bakre, Nwamaka Chizube Ikegwuonu, Emeka Emmanuel Ezugwu, Abam Rufus, Nengi Alazigha, Egop Brownson Egop, Christian Maduabuchi Eke.
Writing - proofreading and editing: Michael Promise Ogolodom, Chukwuma Martha Chinazo, Anelechi Kenneth Madume, Olukumnmi Ijeruh, Abdul Fatai K. Bakre, Nwamaka Chizube Ikegwuonu, Emeka Emmanuel Ezugwu, Abam Rufus, Nengi Alazigha, Egop Brownson Egop, Christian Maduabuchi Eke.